

Travesty
SAMHSA's New Strategic Priorities Signal Retreat From Role of National Leadership in Behavioral Health

Yesterday, my former employer, the Substance Abuse and Mental Health Services Administration, published the new strategic priorities for the agency under the Trump administration. The new strategic priorities set a new course for SAMHSA under Trump, and it is a course that is grounded in division, stigmatizing rhetoric, and a retreat from meeting Americans where they are at with their behavioral health.
There is no sugarcoating it, the document is a travesty, and marks a sad, sad chapter in the history of an agency, that for decades, has provided national leadership in the behavioral health space, in a manner that was grounded in evidence and empathy, and yes that other evil ‘e’ word, equity. What this means is that the nation’s behavioral health workforce, at least those of us who are still grounded in the ethos of evidence and equity, will have to look elsewhere for that leadership. Or, perhaps, it means we need to build it ourselves.
It is important for me to state and stress there are still many, many, many good people at SAMHSA who are still driven to serve the American people, ALL of its people. I have good, dear friends and colleagues who are still there trying to do the right thing in these trying circumstances. These new strategic priorities are not reflective of the dedicated rank and file staff who remain. But it is reflective of the leadership at HHS, forcing SAMHSA to pivot away from its established legacy of trusted national leadership in all things mental health and addiction. It is inescapable that this new direction will gravely tarnish the reputation of SAMHSA. And even in a new administration that beliefs in behavioral health equity, it will take time to rebuild that reputation.
I want to examine the new strategic priorities and contrast with the previous priorities set in the Biden administration, however, first I have a couple of reflections of the Executive Summary and write up of the new principles. Those reflections are on the topics of language and hypocrisy.
You can find the announcement and description of SAMHSA’s new priorities published at this page: https://www.samhsa.gov/about/strategic-priorities
Language
What is immediately noticeable in the write up for the new priorities is the new language of SAMHSA. For starters, it is abundantly clear that “abuse” is back. The word “abuse” is used ten times. This, is a clear signal that this administration has determined that “substance use disorder” is too “woke”, and that it is requiring SAMHSA to return to stigmatizing language and policies. One could not even describe the tone as “tough love”, because there is not an ounce of empathy communicated nor implied in the description of the new direction and priorities.
The tone is clearly combative, and it starts in the very first paragraph of the executive summary (italics and bolding for emphasis by me):
This document provides a detailed overview of SAMHSA’s strategic priorities. Through these priorities, SAMHSA will lead the Department’s efforts in changing the trajectory of increasing serious mental illness, addiction, and loss of life. SAMHSA will no longer be sidetracked by misguided policies, investments in unsupported clinical interventions, and any unlawful focus on specific populations.
Of course given the Administration’s war on everything DEI, this direction is not a surprise. However it is very jarring to see it in a document written by SAMHSA and published on the SAMHSA website, when for years, health disparities and behavioral health equity have been a focus of SAMHSA’s work. Indeed, when I wrote the initial application and reapplication for the New England Prevention Technology Transfer Center, in both applications we were required to submit health disparity statements and describe how we would address health disparities. That first application was during the first Trump administration. So yes, this language is very jarring to see on a SAMHSA webpage.
Hypocrisy
There are two passages that really struck me, that demonstrated a deep level of hypocrisy and self-contradiction. First, there is this passage in the section describing the mental health and addiction issues facing our country, in particular our children (again, emphasis mine):
In addition, the proliferation of social media and other technology that is inundating America’s young people, coupled with other social stressors in homes and communities across the Nation, have contributed to declining mental health and well-being and rising rates of suicide.
Real talk, right now, a major source of stress in homes and communities across the Nation originates with our government. The draconian and authoritarian tactics of ICE and DHS have caused immense amounts of stress for communities and families. The bullying of LGBTQIA+ Americans by this administration, through its policies and public-facing language is imposing stressors in homes and communities. The mass firings of tens of thousands of federal employees, like myself, is causing stress and anxiety for many households across the nation. Now is a time when we need our national agency for mental health advocating against policies that are going to adversely impact the mental health of Americans, but alas, HHS leadership is certainly not going to allow such a thing.
Towards the end of the document, SAMHSA spells out how the agency will be ending DEI. To be clear, DEI at SAMHSA was all but ended on January 20th when we were put under immediate communication and external engagement freeze and the quickly issued Executive Order on ending DEI. From the time that was issued, many SAMHSA resources and webpages were taken down permanently, or scrubbed of anything that could be perceived to be DEI. This priority document makes it official that SAMHSA is not just ending DEI, it will now officially be anti-DEI.
To the extent permitted by law, SAMHSA will deprioritize diversity, equity, and inclusion (DEI) initiatives, which prioritize group identity over individual merit. We believe opportunities should be based on character, effort, and ability, not race or other group identity. SAMHSA is committed to restoring merit-based opportunities and removing unlawful discriminatory practices, (including unlawful proxies for racial discrimination).
SAMHSA has previously invested substantially in ideologically laden concepts like behavior health equity and focused on health disparities—mainly on identifying and documenting worse health outcomes for minority populations. This has not translated into measurable improved health for minority populations, and in many cases has undermined core American values.
SAMHSA will prioritize efforts that go beyond addressing health disparities to focusing on solution-oriented approaches. This includes actively testing, advancing, scaling, and implementing innovative evidence-based interventions and treatments that address poor health outcomes, including the root causes of Americans’ chronic disease epidemic.
Just linger on that one phrase for a moment: “…and in many cases has undermined core American values.” What does that mean? SAMHSA is now saying that the work the agency did, to develop culturally responsive behavioral health services and to encourage culturally responsive behavioral health systems “undermined core American values.” What exactly is “un-American” about an American receiving the care that is most aligned with their cultural experiences and values around behavioral health? Moreover, the authors of these new strategic priorities are not showing their work. What is the evidence that culturally responsive services have not translated into results? This is shameful and a sad chapter for SAMHSA’s legacy, one I know was most likely not actually written by the good people who remain at SAMHSA.
The other observation about this section of the strategic priorities is that it is self-contradictory. It is decreeing that SAMHSA will now ignore health disparities but instead put focus on testing interventions and strategies for the root causes of behavioral health issues. But, health disparities ARE a root cause influencing outcomes such as overdose rates.
This all said, another important phrase in this section is this one, “To the extent permitted by law”. It is my hope that states and national advocacy groups in the various domains of behavioral health will challenge the administration when (not if), it illegally forbids states from using their federal resources to fund behavioral health services and systems that are culturally responsive. If you are a black American taxpayer, you deserve to be served by programs that are going to be most responsive to your behavioral health needs. You should not be made to settle for only programs and services that have only been tested and validated on white populations. That is a disservice. And I’m no lawyer but it seems like if it isn’t, it should be illegal.
Priorities and Cross-Cutting Principles
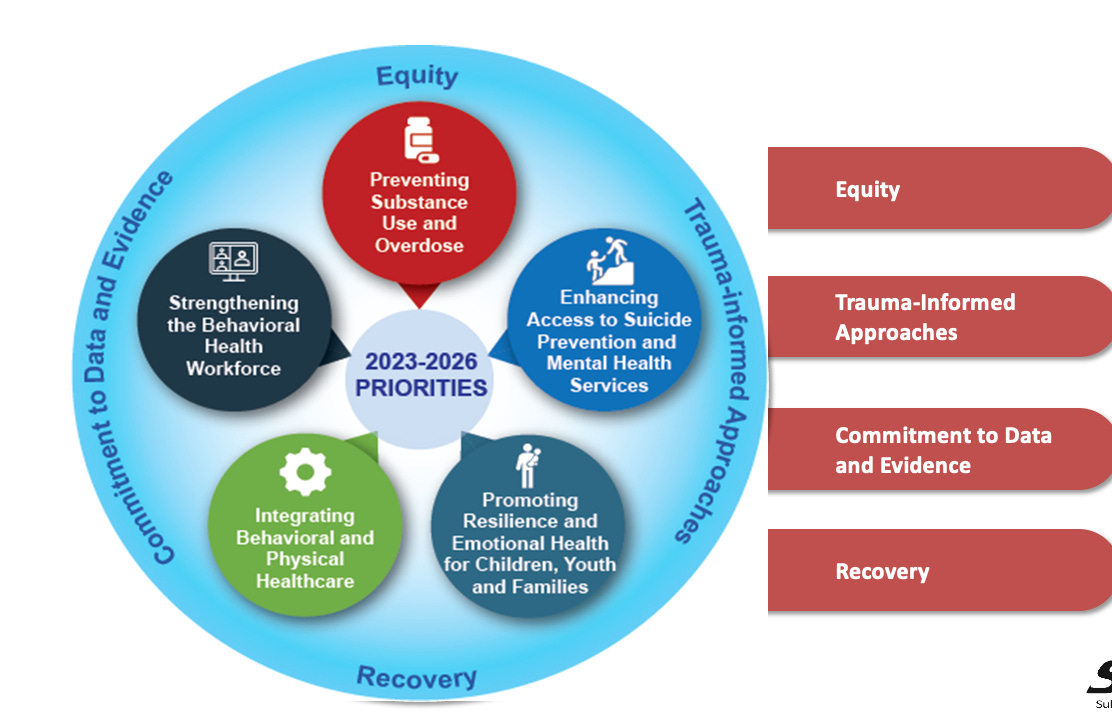
I suspect I will be writing many essays in the coming months on how these new strategic priorities will manifest into grants, programs, and resources coming from SAMHSA, but let’s take a high-level look at the new priorities. The chart below comes from the announcement.

One comment purely on aesthetics, the previous priorities looked so much nicer. That bottom hexagon in the infographic above just has WAY too many words crammed into it. For comparison, the previous priorities below:
At first reading, some of the new strategic priorities read like valid priorities for behavioral health.
Preventing substance misuse and addiction? Sure.
Identifying and addressing emerging behavioral health threats? Uh, not a fan of the aggressive language, but sure, we should be identifying and addressing emerging needs and challenges.
But then we get into the problematic priorities. There is this one where it feels like they came up with the title of the priority and then just mailed it in. This literally is the title and summary of this priority:
Expanding Crisis Intervention Services
Historically, mental health crisis services in the U.S. have been inconsistent and inadequate. SAMHSA will prioritize strong partnerships between crisis care systems and law enforcement (and other first responders), which are essential for public safety, including suicide prevention.
Vague. Little details. Who knows what this will actually mean in practice?
Then there is this priority:
Helping individuals achieve long-term recovery and sobriety,
This priority and the language that goes along with it is worrying, but not surprising. We already knew this administration has rejected harm reduction and is actively routing it out of all programs and services. However, with the inclusion of the word “sobriety” what we will need to pay attention to is how this strategic priority impacts services such as recovery housing. Will there be strict new standards for individuals seeking to use federally funded recovery housing? Will people be immediately kicked out if they experience a relapse? What about states with legal adult-use and medical cannabis laws, will medical cannabis patients who are also in recovery substance use disorder be forbidden from federally funded recovery housing?
SAMHSA goes on to describe how they will actualize these strategic priorities, and…well…they read like they were written by a college student cramming to finish a paper the night before it was due:
To advance the Agency’s Mission and Six Strategic Priorities, SAMHSA has identified five core areas of work:
Analyzing and Disseminating Information on the Latest Data, Trends, and What Works in Prevention, Treatment, and Recovery
Building Capacity and Provision of Services at the National, State, Tribal, Territorial, and Local Levels Through Strategic Resource
Advancing Behavioral Health Through Strategic Collaborations and Partnerships
Engaging in Education and Communication Efforts to Catalyzing Action
Testing and piloting innovative solutions that solve long-standing problems, replicate successes, and eliminate ineffective programs
What the heck does this mean? “Building Capacity and Provision of Services at the National, State, Tribal, Territorial, and Local Levels Through Strategic Resource” it’s not even a complete thought. Additionally, “Engaging in Education and Communication Efforts to Catalyzing Action” is word salad. This is the sort of thing that would be written by some senior HHS leader who doesn’t really understand what SAMHS is supposed to do but strings together some words that sound smart. I’ve seen several instances of this administration using some version of “catalyzing”, it seems to be one of their preferred buzzwords that means not much of anything. The language used throughout this document is miles away from the care, skill, and professionalism displayed in the write up for the previous 2023-2026 strategic priorities and strategic plan, and other SAMHSA resources and announcements.
One final comment, for now, is that in the cross-cutting principles we see Secretary Kennedy’s favorite phrase “Gold Standard Science”. To date, I’ve seen (too much) of his testimony in Congress and I’ve yet to hear him clearly define and articulate what this actually means in practice. All I know is this is the same man who set a pre-determined date at the end of September to find and announce the cause of Autism, so whatever his definition may be of “Gold Science” color me highly skeptical that it is a form of science that has even an ounce of reliability.
The Road Ahead
This indeed marks a very sad and unfortunate chapter in the history of SAMHSA. Throughout my nearly 20-year career in the prevention field, I’ve long had some connection to SAMHSA. I’ve coordinated local prevention programs funded by SAMHSA dollars, I served on SAMHSA’s Center for Substance Abuse Prevention National Advisory Council, I’ve helped develop SAMHSA resources, I was the founding Director of the SAMHSA-funded New England Prevention Technology Transfer Center, and of course most recently I was a SAMHSA employee as the New England SAMHSA Regional Director. As with any organization and entity, they weren’t always perfect, I didn’t always agree with everything SAMHSA did, or didn’t do, but I can safely say the throughline has been one of an agency driven by science and by working towards increasing effective behavioral health programs and services for all populations.
Never, in all of that time, could I have imagined SAMHSA being forced to disown a substantial part of that legacy, and to not just disband, but become antagonistic to, the cause of behavioral health equity and addressing behavioral health disparities. Yet, here we are. I feel for all of the good people left at SAMHSA who are being forced into this new paradigm. I feel for all of the state, tribal, and territorial behavioral health leaders who have to navigate this new paradigm. And I feel for the many communities who are being abandoned.
Filling the Void
In the end, there is a huge void of leadership in behavioral health that needs to be filled. Perhaps we can take a lesson from the states here in the Northeast who have organized to address the void left by the U.S. CDC in the area of vaccine guidance. Previously, I wrote about and proposed a vision for national behavioral health policy to counter the Trump plan to return to cuffs and cages. Our communities still need support, guidance, and leadership in behavioral health, with a focus on equity and culturally responsive services. I would submit this is an opportunity for alternative leadership to organize and emerge and provide that leadership and direction.
The new direction from SAMHSA is indeed a travesty, but we can’t just live with this reality.
Let’s band together to rewrite it!
-Scott, The Radical Preventionist